

ENTER LABEL TEXT
Use your most relevant and current information.
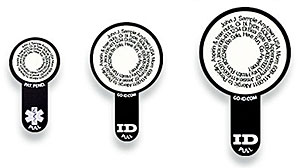
Top Arc: Start with your name, date of birth
Center Lines:
- City, State, Country
- Medical Condition or allergy(s)
- Medication(s), Surgery(s)
- Medication(s),or blood type,weight if child
- Insurance provider & number
- Emergency contact(s) 2 or more
- Inspiring message
Bottom Arc: Emergency Contact #1 or #1 Medical condition or allergy
Use your most relevant and current information.
For example, begin with your name and date of birth, followed by your emergency contact, then your city, state, country, medical conditions*, allergies, medications, blood type, weight(if child), health insurance provider and number**.
CLICK HERE for information recommendations and suggested abbreviations.
After entering your information, click the button to update your preview.

PREVIEW





{kind=link}